Attention Members: Please avoid clicking on any unsolicited emails with attachments. If you have any concerns, please contact us at info@veteducation.com.au for clarification.
Attention Members: Please avoid clicking on any unsolicited emails with attachments. If you have any concerns, please contact us at info@veteducation.com.au for clarification.
Updates in Understanding Acute Pancreatitis in Dogs and Cats: 2010-2020
Philip R Judge BVSc MVS PG Cert Vet Stud MACVSc (Veterinary Emergency and Critical Care; Medicine of Dogs)
What Is Pancreatitis?
Acute pancreatitis is a potentially life-threatening disease characterized by inflammation of the pancreas, and uncontrolled activation of pancreatic enzymes and cellular damage. Systemic dissemination of pancreatic enzymes and mediators of tissue inflammation lead to the development of systemic inflammation and widespread organ dysfunction1. Acute pancreatitis is associated with the development of sepsis and multiple organ dysfunction syndromes, in both humans and animals. Additionally, pancreatitis is a known predisposing condition in the development of acute kidney injury, acute respiratory distress syndrome, disseminated intravascular coagulopathy, cardiac dysfunction, and intestinal dysfunction1,2.
The diagnosis and management of pancreatitis in small animal patients can present several challenges, including how to control pancreatic inflammation, and support the patient during therapy.
What Causes Pancreatitis?
To date, there are very few established causes of pancreatitis in dogs and cats. There are however several known risk factors or associations, including the following1,2.
1. Metabolic Associations a. Obesity b. Severe intestinal disease c. Diabetes mellitus d. Hyperadrenocorticism e. Hyperlipidaemia f. Fatty food ingestion. g. Kidney insufficiency h. Pancreatic duct obstruction i. Immune-mediated (as result of chronic pancreatitis) 2. Pancreatic ischaemia caused by trauma, and other causes of ischaemia 3. Infection – infectious agents implicated in the development of pancreatitis in dogs and cats include a. Feline infectious peritonitis b. Toxoplasmosis c. Ascending bacterial infection originating in the gastrointestinal tract. This is reported with regularity in human literature but appears an uncommon cause in dogs and cats.
4. Toxins and Drugs: There are many drugs and toxins that are documented as potentially contributing factors in the development of pancreatitis, including… a. Azathioprine b. Chlorothiazide c. Hydrochlorothiazide d. Zinc e. Potassium bromide f. Vinblastine g. Sulfonamides h. Cisplatin i. Organophosphates j. L-asparaginase k. 5-aminosalicylateAlcohol l. Azathioprine m. Oestrogen n. Tetracycline o. Furosemide p. Thiazide diuretics q. Chlorpromazine
In addition to the aforementioned, increasing age and being de-sexed/neutered are also suspected risk factors.
The Pathophysiology of Acute Pancreatitis
The first step in the development of acute pancreatitis involves pancreatic acinar damage. The second involves activation of digestive enzymes within the gland, with resultant pancreatic auto-digestion. Thirdly, inflammation occurs in tissues in which damage has occurred. Finally, systemic dissemination of activated pancreatic enzymes and inflammatory mediators contributes to the systemic inflammatory response seen in many patients with pancreatitis1,2.
Damage to acinar cells may be predisposed to by any of the factors mentioned above, including trauma, shock, and high fat diets, although much of the evidence supporting some these causes still remains speculative at present1,2. As described above, once pancreatic tissue has been damaged, a cascade of inflammatory events occurs, compounded by activation of pancreatic enzymes, and dissemination of the inflammatory mediators into the systemic circulation. Interestingly, pancreatic enzymes are probably not essential early in the pathogenesis of pancreatitis. However, once enzyme activation has occurred, the normal pancreatic defense mechanisms, such as pancreatic secretory trypsin inhibitor, become overwhelmed, and enzyme activity within the pancreas contributes significantly to local tissue damage2.
In addition to multiple cytokines being stimulated, there is an alteration in pancreatic circulation that exacerbates inflammation. Necrotizing pancreatitis causes a progressive reduction in capillary flow after acinar cell injury that cannot be reversed by fluid resuscitation alone in experimental models. Additionally, the intestine is thought to contribute to or exacerbate inflammation directly due to intestinal ischemia2.
Clinical Signs of Acute Pancreatitis
The clinical signs associated with pancreatitis are frequently non-specific. They can also vary in intensity and severity from mild to severe. The majority of severe symptoms result from significant local and systemic dissemination of inflammatory mediators from the inflamed pancreas1,2.
The most common symptoms include loss of appetite, abdominal pain, vomiting, and obtundation. Other clinical signs evident on patient assessment and examination can include1,2:
Respiratory symptoms: Tachypnoea and/or respiratory distress may result from abdominal discomfort, fever, aspiration pneumonia or acute lung injury caused by circulating inflammatory mediators2
Cardiovascular symptoms: Shock may result from acute fluid loss into the gastrointestinal tract, or maldistribution as a result of systemic inflammation. Additionally, fluid loss and reduced fluid intake may cause dehydration. Systemic inflammation, pain and electrolyte abnormalities may also result in cardiac arrhythmias1,2.
Coagulopathy. Coagulation abnormalities are common in patients with pancreatitis, with the most common coagulation abnormality being disseminated intravascular coagulopathy (DIC) as a result of systemic inflammation.
Gastrointestinal Symptoms: In addition to vomiting and reduced food and water intake, some patients may develop intestinal ileus and diarrhoea
Neurological/Behavioral Symptoms: Obtundation is common in acute pancreatitis. Acute electrolyte disturbances can result in seizures or development of stupor and coma
Miscellaneous Symptoms a. Fever may be present due to the systemic release of mediators of inflammation b. Jaundice may occur with concurrent obstruction of common bile duct, neoplasia, and swelling or obstruction/spasm of the sphincter of Oddi. c. Presence of pleural fluid
The Diagnosis of Acute Pancreatitis
Pancreatitis can be a difficult disease to diagnose, and currently no single test can reliably diagnose pancreatitis in all cases. In some patients, to definitively diagnose pancreatitis requires direct visualization of the pancreas +/- a pancreatic biopsy and histopathology. However, there are some clues that can be obtained from routine biochemistry, haematology and immunological testing, along with diagnostic imaging that can assist the clinician to form a clinical diagnosis of pancreatitis, even if definitive diagnosis remains elusive1-3.
Serum Biochemistry Alterations in Acute Pancreatitis
Amylase and lipase elevations: Both amylase and lipase enzymes originate from the pancreas, but also intestinal mucosa, and liver1,2. Serum levels therefore, may increase in pancreatitis, but also with other causes of gastroenteritis. Both enzymes have very short half-life in serum (4-6hrs) and so levels may be normal when tested even if pancreatitis is present. In addition, both enzymes excreted by kidneys, and may be elevated with kidney disease, pre-renal conditions, and post renal obstruction1-3
Lipase has a sensitivity ranging between <50% and 73%, meaning up to 50% of patients with pancreatitis will have normal lipase levels. Lipase has a specificity of 55%; meaning 45% of cases with elevations in lipase have no pancreatic disease (such as with malignancy, intestinal, kidney, or hepatic disease).
Two recent studies showed normal amylase in 30-50% and normal lipase in 60% of dogs with histologically confirmed pancreatitis, highlighting the low sensitivity of these enzymes for detecting pancreatitis.
However, in a cohort of patients with elevated amylase, a study found elevations in amylase of greater than 1400 U/L had a sensitivity of 68.9% and specificity of 81.8% for acute pancreatitis4.
Pancreatic Lipase Immuno-reactivity (PLI) – In contrast to catalytic assays for the measurement of lipase activity, use of immunoassays allows for the specific measurement of lipase originating from the exocrine pancreas5,6. The most commonly used tests are an enzyme immunoassay (cPL; fPL) and a sandwich enzyme-linked immunosorbent assay (Spec-cPL; Spec-fPL)5-6.
Canine cPL and Spec cPL are frequently elevated in dogs with pancreatitis. The cPL ELISA test has a reported sensitivity in various studies ranging between 64% and 82%, with a reported specificity of 80-97%. Both cPL and Spec cPL have increasing sensitivity with increasing severity of disease1-3.
Using Spec-cPL, results <200 µg/L are expected in healthy dogs, and results >400 µg/L are considered consistent with a diagnosis of pancreatitis2,5.6.
The reference interval for the Spec fPL assay is 0-3.5 mg/L, and concentrations more than 5.3 mg/L are considered consistent with pancreatitis5.
An in-clinic rapid semiquantitative assay (SNAP-cPL; SNAP-fPL, IDEXX, Maine, USA) has also been developed for dogs and cats, and shows good alignment and reproducibility with both Spec-cPL and Spec-fPL2,5. In a review of the accuracy of SNAP-cPL tests in dogs, the assay was found to have a sensitivity of between 91 and 94%5. In another study of 38 dogs with acute abdominal disease, the SNAP cPL test had a sensitivity of 82%, but a specificity of only 60% – underlying the importance of not basing a diagnosis of acute pancreatitis on a single test5
Feline Spec-PLI (fPLI) – this test, similar to the cPLI test has a reported sensitivity of 79% and a reported specificity of 80%. It is currently considered the most sensitivity test for pancreatitis in the cat5.
Canine C-reactive protein (CRP) – CRP is an acute-phase protein produced by the liver in response to macrophage-derived and adipocyte-derived factors in inflammation7. Its physiological role is to bind to phosphocholine expressed on the surface of dead or dying cells (and some types of bacteria) in order to activate the complement system. Although not specific for pancreatitis, increased levels of C-reactive protein were found in circulation of patients with necrotizing pancreatitis in one animal study4,6. In a retrospective study of 64 dogs with acute pancreatitis, C-reactive protein concentrations significantly reduced during treatment of acute pancreatitis, and may be used as a marker for resolving disease. The quantity and rate of CRP reduction did not correlate with any difference in duration of hospitalisation in this study4,7.
Other biochemical abnormalities seen in patients with pancreatitis include
Acute pancreatitis can result in elevations in alanine transferase (ALT), aspartate transferase, glucose, serum triglycerides, calcium (which may also be normal or decreased), and alkaline phosphatase4. In one study, sustained elevations in ALT were associated with longer hospital stays, but had no relationship with mortality4.
Decreases in albumin may be present in the acute phase (negative acute-phase protein) and late phase of disease (due to systemic inflammation)2.
Elevations in serum creatinine >212 µmol/L were found to be significantly associated with poor outcome and death (odds ratio 12.5) in one study of 50 dogs with acute pancreatitis8. Likewise, azotemia was associated with a higher risk of death in dogs with acute pancreatitis8.
Serum sodium concentrations < 139 mmol/L are associated with worse outcome (odds ratio 4.9), evidenced in the same study of 50 dogs with acute pancreatitis8.
Haematological Abnormalities in Acute Pancreatitis
Haematology may show an elevated haematocrit due to haemoconcentration, dehydration, and splenic contraction. A leucocytosis with left shift is common but is not always present, and is not associated with non-survival8.
Radiography
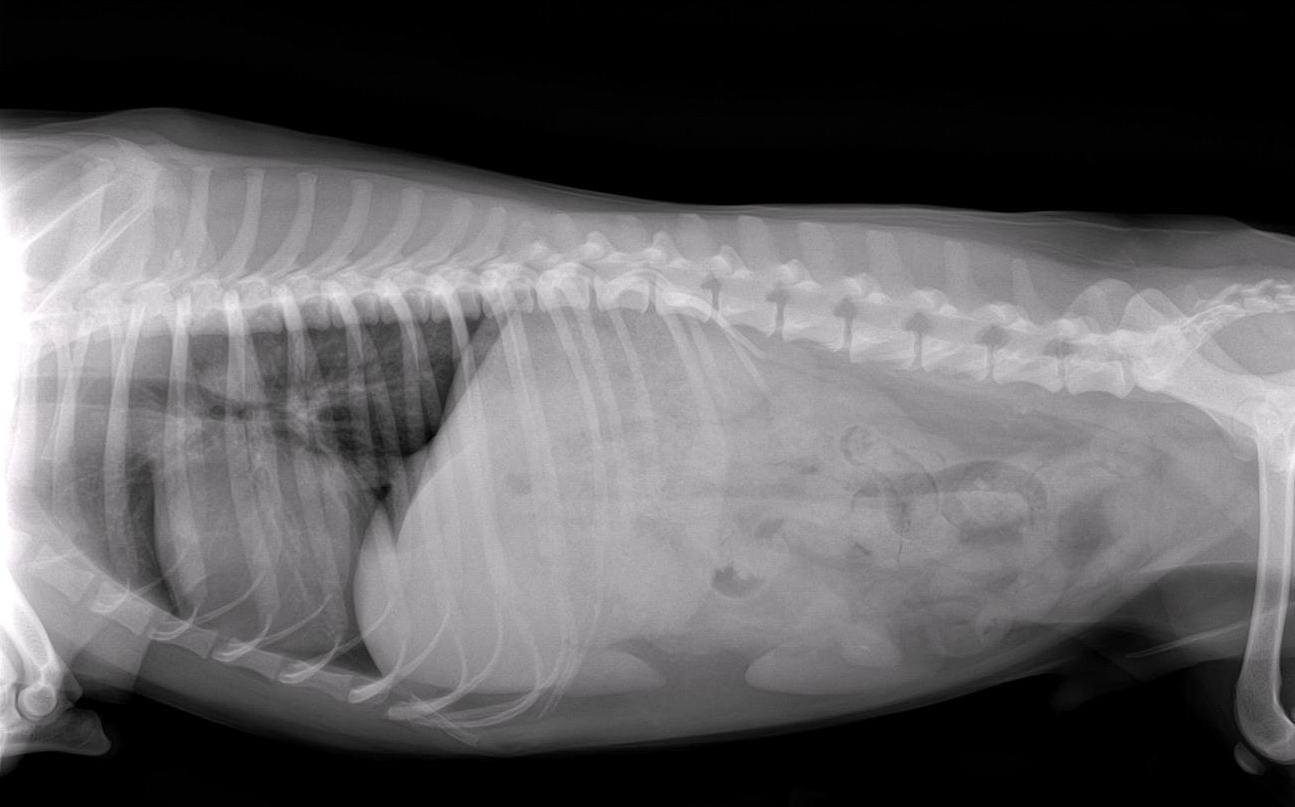
Radiography of the abdomen is recommended in all patients suspected of intra-abdominal disease. However, abdominal radiography may be normal in up to 22-76% of cases of pancreatitis2.8. It’s principle clinical use may be in excluding other diseases that cause similar clinical signs to those of acute pancreatitis9
Classically, the right cranial quadrant shows a loss of detail, and a so-called “ground glass” appearance. In addition, there may be displacement of the duodenum to the right, with the pyloric antrum being displaced to the left. There may also be a static duodenal or colonic gas pattern consistent with intestinal ileus2,9.
Lateral radiograph of a dog with acute pancreatitis. Note the loss of serosal detail in the anterior abdomen. It is important to note that this finding is not specific for acute pancreatitis.
Ventro-dorsal radiograph of a dog with acute pancreatitis. Note the right lateral displacement of the duodenum and the left displacement of the pyloris in this view.
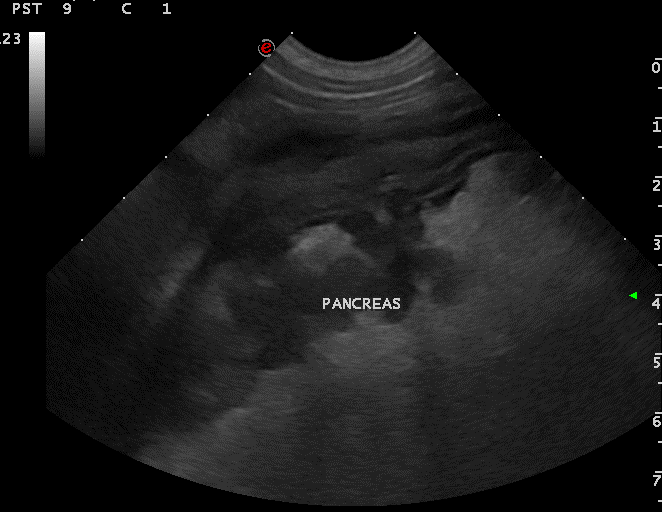
Abdominal Ultrasonography
The diagnostic accuracy of ultrasound for the diagnosis of pancreatitis can approach 90% but is somewhat dependent on operator skill9. The sensitivity of abdominal ultrasound for detection of acute pancreatitis varies considerably, but is reported to be 68% in dogs, and between 11-67% in cats, based on available studies9. Early ultrasound findings in pancreatitis include increasing echogenicity of peri-pancreatic tissue, associated with necrosis and saponification of peri-pancreatic tissue, surrounding hypoechoic, oedematous pancreatic tissue. Formation of cysts, abscesses or pseudocysts within the pancreas can lead to the presence of anechoic regions within the pancreas1,2.
Interestingly, in a study of ultrasound evaluation of acute pancreatitis on 38 dogs, sensitivity of ultrasound-diagnosis increased when ultrasound was performed 48-hours after admission, suggesting repeated ultrasound assessments be conducted where results of an initial ultrasound are inconclusive10.
In some cases, the development of local regions of inflammation and peritonitis around the pancreas can markedly reduce ultrasound image sensitivity, and can make a specific ultrasound diagnosis difficult and perhaps presumptive at best in these circumstances2.
Diagnostic Peritoneal Lavage (DPL)
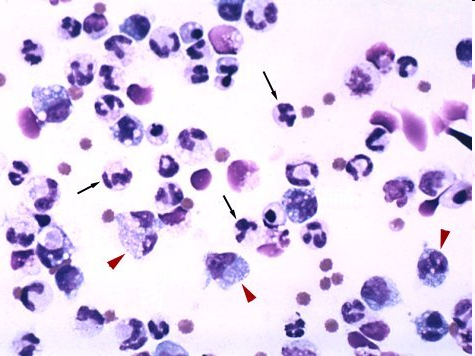
DPL may reveal a serosanguinous fluid, elevated leukocyte count, and degenerate neutrophils. The amylase and lipase concentration of abdominal effusion, if measured, is always more elevated than serum levels, and this can be a helpful diagnostic test if results of other tests are equivocal
Free abdominal fluid sample from a dog with pancreatitis showing large numbers of neutrophils, many of which have vacuolated cytoplasm.
Contrast-Enhanced CT
CT can be used as a diagnostic tool for visualizing pancreatic tissue and surrounding structures. However, the test is not always readily available, is limited by cost, and the requirement for patient general anesthesia. Additionally, studies of CT in acute pancreatitis to date have shown low sensitivity in dogs and cats9. CT angiography (CTA) is another technique used in humans with acute pancreatitis. In a single study in dogs, CTA better identified portal vein thrombosis than abdominal ultrasound, and this may be of significance in therapeutic decision-making in affected patients11.
CT of the pancreas in a dog with pancreatitis.
The Treatment of Acute Pancreatitis
There is no specific therapy targeted at pancreatitis. The management of pancreatitis is thus largely supportive in nature, and falls broadly into three categories
Restoration of normal fluid, electrolyte and acid-base status
Nutritional support of the patient
General supportive care of the patient and vital organ systems
Correction of fluid, electrolyte and acid/base imbalances
Fluid loss into third spaces such as the gut, abdominal cavity, interstitial spaces, lung and pleural space can be significant in the patient with acute pancreatitis1,2.
Hypovolaemia should be corrected within the first hour of presentation, using a balanced, buffered electrolyte solution such as lactated Ringer’s solution. The goal of treatment of hypovolaemia should be to optimize tissue oxygen delivery by normalizing cardiovascular parameters, such as blood pressure, heart rate, and other perfusion indices, as well as optimizing PCV at or above 27%1,2.
Following acute volume resuscitation, isotonic crystalloids should be used to provide for rehydration and maintenance, and thereafter (12-24hs) provided at rates to cover maintenance fluid requirements, plus ongoing losses only.
Fresh frozen plasma has been recommended for use in acute pancreatitis for many years. However, in both human and veterinary studies, there is no apparent survival benefit in patients receiving plasma for reasons other than maintenance of serum albumin concentration2.
Feeding the patient with pancreatitis
Traditional recommendations for nutrition of patients with pancreatitis have centered around providing bowel rest, and providing parenteral nutrition. However, parenteral nutrition in patients with pancreatitis has many complications, and produces longer hospital stays, and higher rates of infections, and is not associated with improved survival, and, at present, lacks evidence-based benefit2,12-15.
Recently, studies evaluating provision of early enteral nutrition in patients with pancreatitis has been shown to shorten hospital stay, results in lower incidence of sepsis and infection, and a more rapid resolution of elevated markers of inflammation2,12-15.
The optimal route for enteral nutritional support in patients with pancreatitis is thought to be via the jejunum, followed by the duodenum, and the stomach. Interestingly however, a recent study in humans found no difference in clinical outcome or biochemical markers for pancreatitis when using naso-gastric versus jejunostomy feeding tubes. In addition, two recent studies, one of 55 cats, and another in 10 dogs with pancreatitis showed patients tolerate nasogastric feeding well, with few complications, suggesting that orogastric feeding may be able to be utilized effectively in patients with pancreatitis2, 12-15.
In general, the following recommendations can be made regarding nutritional support of the patient with pancreatitis
For the first 12-18 hours of hospitalization – begin micro-enteral nutrition by the oral route, or by naso-oesophageal tube. Micro-enteral nutrition involves the feeding of glucose, glutamate, glycine and electrolyte solutions at a rate of 1-2 ml/kg/hr. These solutions provide a ready substrate for gastrocytes, and are shown to improve gastric mucosal health, and tolerance to more complex diets that are subsequently fed16.
From 12-18-hours onwards – feed a hydrolyzed liquid diet, at a rate of 1-2 ml/kg/hr either by naso-esophageal tube, or by surgically placed jejunostomy tube (if the patient is vomiting or is not tolerating oral or naso-esophageal feeding) while continuing oral administration of micro-enteral nutrition. The patient should receive 1/3 of resting energy requirements (RER) on the first day of feeding, 2/3 resting energy requirements on day 2 of feeding, and the entire caloric requirement for RER on day 3 of feeding.
Nutritional support should ideally begin within 12-24 hrs. of hospitalisation, to mitigate the catabolic effects of critical illness. The ideal diet for nutrition of patients with pancreatitis is unclear. Typically, low-fat, carbohydrate-rich diets have been advocated. However, there is little evidence of outcome advantage over feeding a higher fat diet in acute pancreatitis. There are a few ongoing trials being conducted at present to determine the optimum diet for dogs with acute pancreatitis12-15.
In cats, the same principles may be applied – however it is even more important to avoid fasting in cats with pancreatitis, as this is associated with the development of severe hepatopathy (hepatic lipidosis) and a deterioration of clinical signs. In addition, vomiting is less associated with pancreatitis is cat, making them perhaps better candidates for tolerating naso-esophageal feeding tubes17.
Ancillary measures and general patient support.
Measures that may be beneficial in the management of the patient with acute pancreatitis include the following
Antibiotics – the use of antibiotics in patients with pancreatitis is controversial in dogs and cats, due to the low incidence of infection as a causative or complicating factor in the disease. Every effort should be made to identify the causative organism if an infectious agent is suspected, prior to commencement of antibiotic therapy. The use of antibiotics may be beneficial if the patient has clinical signs of sepsis, or infection1,2. Bactericidal antibiotics are preferred. Enrofloxacin or beta-lactam antibiotics are generally preferred empirical choices.
Analgesia should be provided with an opiate analgesia12. Pain has a negative effect on parasympathetic blood flow to the pancreas, and is associated with sustained sympathetic nervous system stimulation, and the development of abnormal blood pressure, oxygen delivery to tissues, with subsequent organ damage. Fentanyl is preferred, as it can be readily be administered by continuous infusion, resulting in superior analgesia to bolus therapy with medications such as methadone. Morphine may result in contraction of the sphincter of Oddi, and is less preferred over fentanyl in patients with severe abdominal pain, but may be used nevertheless. For patients with severe abdominal pain that persists despite the use of fentanyl, the following additions to opioid analgesia should be considered.
Epidural anaesthesia – in an experimental model of pancreatitis, provision of epidural anaesthesia to animals with pancreatitis resulted in a reversal of sympathetic nervous system and disease-mediated abnormal blood flow through the pancreatic microvasculature
Disseminated intravascular coagulopathy is managed by ensuring the patient has adequate circulating blood volume, haematocrit, blood pressure, tissue oxygenation, and by providing blood clotting factors e.g. fresh frozen plasma when indicated. Current recommendations are to administer fresh frozen plasma to patients with pancreatitis at 10-20 ml/kg q 12-24 hrs in order to supply clotting factors only in the presence of active bleeding, or anticipated invasive diagnostic or therapeutic procedures.
Selenium dosed at 0.1mg/kg slow IV q 24 hrs has shown promising results in improving mortality in one canine study, and warrants further investigation. Currently however, there is little evidence to support the current use of selenium in the management of pancreatitis until further research is performed.
Anti-inflammatory medication: There is no evidence that administration of NSAID’s, including COX-2 selective NSAID’s improve the clinical outcome of patients with acute pancreatitis2,18. Corticosteroids are currently receiving increased attention in human medicine. Recent studies are revealing that short-term high dose hydrocortisone administered early in experimental pancreatitis may improve patient outcome. However, these studies involve models of pancreatitis that do not accurately mimic the disease in dogs and cats, making extrapolation of this data unreliable at present. In addition, corticosteroids may impair the removal of macroglobulin-bound proteases from the plasma by the monocyte-macrophage system, among other catabolic effects. Conversely, however, corticosteroids may increase production of pancreatitis-associated protein, which confers a protective effect against pancreatic inflammation. Corticosteroids may also be beneficial in sepsis, in patients not responsive to vasopressors and inotropes, as some of these patients develop critical-illness-related corticosteroid insufficiency2. A recent study evaluating 65 dogs with acute pancreatitis revealed those treated with prednisolone 1 mg/kg/day had earlier reduction in concentrations of C-Reactive Protein, and earlier improvement in clinical signs over non-prednisolone treated dogs19.
Anti-emetic therapy has not been evaluated in prospective clinical studies in dogs. However, control of intestinal discomfort and nausea is critical to improving patient tolerance of enteral feeding. Experimental models have shown dopamine infusion improves outcome in acute pancreatitis, and reduces the severity of inflammation. Theoretically, there would be a disadvantage to using metoclopramide (a dopaminergic antagonist) – but this is unproven2. Administration of broad spectrum anti-emetics such as dolasetron, ondansetron or maropitant citrate may be recommended in patients with persistent nausea and vomiting2. Persistently vomiting patients may benefit from naso-gastric suctioning of gastric contents every 1-2 hours, although there is currently a lack of supporting evidence for this2.
Gastric Acid Suppression: Administration of gastric acid suppressants has not been shown of clinical benefit in humans, and has not been studied in dogs and cats. If used, proton pump inhibitors, such as pantoprazole, are preferred, as they may reduce inflammatory changes in pancreatic acinar cells2,18.
Anti-inflammatory cytokine treatment – administration of anti-inflammatory cytokines, and hormones such as Somatostatin, and enzyme inhibitors have not shown benefit in large-scale human trials. More research is ongoing into the potential benefit of these molecular-based treatments. Administration of atropine, glucagon, and calcitonin has not shown to be of benefit. Given the extent of the inflammatory cascade in pancreatitis, it seems unlikely that any single anti-cytokine treatment will present significant advantages at present18.
Surgery in Acute Pancreatitis
Surgical drainage and debridement of the patient with acute pancreatitis may be a useful adjunct to standard medical therapy in many patients with severe pancreatitis. Lavage of the abdomen helps to lessen the severity of disease because it removes significant amounts of active pancreatic enzymes, and reduces the burden on the plasma protease inhibitor system. However, the timing of surgical intervention in patients with pancreatitis has remained controversial for many years. Additionally, mortality rates of greater than 50% are reported in veterinary literature, when acute pancreatitis is managed with surgical intervention2.
Cytology of lavage – intracellular bacteria, vacuolated WBC
Amylase of lavage fluid > 200 IU, and increasing
Lipase of lavage fluid > serum lipase, and increasing
As with any surgical procedure in a critical patient, care and attention must be paid to essential organ systems, anaesthetic selection, and appropriate patient stabilization in order to reduce patient morbidity or mortality as a result of the surgical procedure
Complications and Prognosis
Complications of acute pancreatitis can be severe, and include the development of systemic inflammation, sepsis, septic shock, acute lung injury, and death2,20. Two illness severity scoring systems – the canine acute pancreatitis severity (CAPS) and simplified CAPS (sCAPS) have been developed and verified, aiming to provide guidance regarding mortality risk from acute pancreatitis21. The scores are based on four (4) independent risk factors for death in acute pancreatitis: systemic inflammatory response syndrome (SIRS), coagulation disorders, increased creatinine and ionized hypocalcaemia. The simplified CAPS uses respiratory rate instead of SIRS criteria21.
A further study evaluating prognostic indicators for acute pancreatitis revealed azotemia, the presence of local complications, such as ascites, and respiratory complications (acute lung injury) were significantly associated with risk of death22, in addition to the CAPS score risk factors.
The illness scoring systems described above may guide discussions with clients on the severity of illness, clinical decision-making, and prognosis.
Management of the patient with acute pancreatitis requires removal of the inciting cause (if known), and the provision of intensive medical treatment aimed at treating shock, restoring normal tissue hydration and perfusion, providing early enteral nutrition, and being vigilant in monitoring and addressing potential complications of the disease.
In very few patients, exploratory laparotomy can provide benefit in aiding removal of inflammatory cells and debris, resection of diseased tissue, and establishing a route for nutritional support.
References
Watson P. Pancreatitis in dogs and cats: definitions and pathophysiology. Journal of small animal practice. 2015 Jan;56(1):3-12.
Mansfield C. Acute pancreatitis in dogs: advances in understanding, diagnostics, and treatment. Topics in companion animal medicine. 2012 Aug 1;27(3):123-32.
Yuki M, Hirano T, Nagata N, Kitano S, Imataka K, Tawada R, Shimada R, Ogawa M. Clinical utility of diagnostic laboratory tests in dogs with acute pancreatitis: a retrospective investigation in a primary care hospital. Journal of veterinary internal medicine. 2016 Jan;30(1):116-22.
Yuki M, Hirano T, Nagata N, Kitano S, Imataka K, Tawada R, Shimada R, Ogawa M. Clinical utility of diagnostic laboratory tests in dogs with acute pancreatitis: a retrospective investigation in a primary care hospital. Journal of veterinary internal medicine. 2016 Jan;30(1):116-22.
Xenoulis PG, Steiner JM. SNAP tests for pancreatitis in dogs and cats: SNAP canine pancreatic lipase and SNAP feline pancreatic lipase. Topics in companion animal medicine. 2016 Dec 1;31(4):134-9.
Haworth MD, Hosgood G, Swindells KL, Mansfield CS. Diagnostic accuracy of the SNAP and Spec canine pancreatic lipase tests for pancreatitis in dogs presenting with clinical signs of acute abdominal disease. Journal of Veterinary Emergency and Critical Care. 2014 Mar;24(2):135-43.
Sato T, Ohno K, Tamamoto T, Oishi M, Kanemoto H, Fukushima K, Goto-Koshino Y, Takahashi M, Tsujimoto H. Assessment of severity and changes in C-reactive protein concentration and various biomarkers in dogs with pancreatitis. Journal of Veterinary Medical Science. 2017;79(1):35-40.
Marchetti V, Gori E, Lippi I, Luchetti E, Manca ML, Pierini A. Elevated serum creatinine and hyponatraemia as prognostic factors in canine acute pancreatitis. Australian veterinary journal. 2017 Nov;95(11):444-7.
Xenoulis PG. Diagnosis of pancreatitis in dogs and cats. Journal of small animal practice. 2015 Jan;56(1):13-26.
Puccini Leoni F, Pelligra T, Citi S, Marchetti V, Gori E, Puccinelli C. Ultrasonographic Monitoring in 38 Dogs with Clinically Suspected Acute Pancreatitis. Veterinary Sciences. 2020 Dec;7(4):180.
French JM, Twedt DC, Rao S, Marolf AJ. Computed tomographic angiography and ultrasonography in the diagnosis and evaluation of acute pancreatitis in dogs. Journal of veterinary internal medicine. 2019 Jan;33(1):79-88.
Mansfield CS, James FE, Steiner JM. A pilot study to assess tolerability of early enteral nutrition via esophagostomy tube feeding in dogs with severe acute pancreatitis. J Vet Intern Med 25[3] May 01, 2011: 419-25
Mansfield C, Beths T. Management of acute pancreatitis in dogs: a critical appraisal with focus on feeding and analgesia. Journal of small animal practice. 2015 Jan;56(1):27-39.
Jensen KB, Chan DL. Nutritional management of acute pancreatitis in dogs and cats. Journal of veterinary emergency and critical care. 2014 May;24(3):240-50.
Harris JP, Parnell NK, Griffith EH, Saker KE. Retrospective evaluation of the impact of early enteral nutrition on clinical outcomes in dogs with pancreatitis: 34 cases (2010–2013). Journal of Veterinary Emergency and Critical Care. 2017 Jul;27(4):425-33.
Ackerman N. Critical care nutrition and supportive feeding methods. The Veterinary Nurse. 2019 Mar 2;10(2):84-9.
Klaus JA, Rudloff E, Kirby R. Nasogastric tube feeding in cats with suspected acute pancreatitis: 55 cases (2001–2006). Journal of Veterinary Emergency and Critical Care. 2009 Aug;19(4):337-46.
Kambhampati S, Park W, Habtezion A. Pharmacologic therapy for acute pancreatitis. World journal of gastroenterology: WJG. 2014 Dec 7;20(45):16868.
Okanishi H, Nagata T, Nakane S, Watari T. Comparison of initial treatment with and without corticosteroids for suspected acute pancreatitis in dogs. Journal of Small Animal Practice. 2019 May;60(5):298-304.
Vrolyk V, Wobeser BK, Al-Dissi AN, Carr A, Singh B. Lung inflammation associated with clinical acute necrotizing pancreatitis in dogs. Veterinary pathology. 2017 Jan;54(1):129-40.
Fabrès V, Dossin O, Reif C, Campos M, Freiche V, Maurey C, Pilot‐Storck F, Desquilbet L, Benchekroun G. Development and validation of a novel clinical scoring system for short‐term prediction of death in dogs with acute pancreatitis. Journal of veterinary internal medicine. 2019 Mar;33(2):499-507.
Kuzi S, Mazor R, Segev G, Nivy R, Mazaki‐Tovi M, Chen H, Rimer D, Duneyevitz A, Yas E, Lavy E, Aroch I. Prognostic markers and assessment of a previously published clinical severity index in 109 hospitalised dogs with acute presentation of pancreatitis. Veterinary Record. 2020 Jul;187(2):e13-.
Learn all about the the basic principles of genetic testing, sample collection, reliable database information, test result interpretation, and recommendations for clients.
This article will explore the presentation, pertinent pathophysiology, patient selection, treatment considerations and outcomes of medical management of canine pyometra.
This short review will focus on the concept of oxygen toxicity, and its relevance in the treatment of the trauma patient - many of whom require and are given oxygen therapy as part of their treatment regime.